
CAPTION: Clinicians have realized that not everyone is a candidate for total knee replacement just because an individual has pain and disability. Many patients affected by knee OA can improve function, reduce pain, and increase range of motion with physical activity and physical therapy.
By Joseph A. Zeni, Jr, PT, PhD
Knee osteoarthritis (OA) is one of the most common knee disorders. Although we often think of knee OA as a disease of the cartilage, OA affects many of the structures in and around the knee joint. With advances in imaging and biomechanics, along with research findings from large epidemiological datasets, we have learned much more about how this disease affects the whole joint in recent years. Patients early in the course of the disease can develop changes to the underlying bone, including bone marrow lesions and sclerosis of the subchondral bone. Even before the cartilage begins to visibly deteriorate on X-rays, advances in Magnetic Resonance Imaging have revealed changes to the cartilage structure that make it less gelatinous and more susceptible to damage. As OA progresses, there are also distinct morphological changes to the muscle, which lead to altered motor control and muscle weakness.
OA Risk: A More Informed View
We have also learned much more about how biomechanics influence the development and progression of OA. Although OA is often referred to as a “wear and tear condition,” only particular types of motion and forces seem to increase the risk for a patient developing OA. Repetitive squatting and kneeling put patients at greater risk for developing OA, but patients with a history of running do not show an elevated risk of developing OA. Abnormal motion in the frontal plane, such as a varus thrust, also increases the risk of worsening OA. This motion occurs when the patient has a quick movement into a bow-legged position when they are walking, running, or climbing stairs. Patients with this type of movement pattern have a three to four times greater risk and faster progression of knee OA than someone who does not have a varus thrust.
Injuries to the anterior cruciate ligament (ACL) and menisci of the knee, particularly those who were treated with a surgical meniscectomy, also appear to be a potential risk factor for developing OA in the future.
“In the past, knee injuries (ie, meniscus tears) went straight for surgery. At the time of surgery, the physician would remove as much of the damaged meniscus as needed. The patient would then develop OA because of the lack of tissue protecting the bones,” says Andrew Vertson, owner/CEO at Intecore Physical Therapy and PT Clinic Metrics, a multi-office practice with several locations throughout Southern California. “Over the past ten years or so, it has become more evident to orthopedic surgeons that leaving as much of the meniscus as possible is the best option to prevent the early onset of OA. Often, the patient would not have surgery but would go directly to physical therapy to strengthen the knee. Research now shows that physical activity, specifically strengthening exercises, to the legs help prevent the significant onset of OA, and physical therapy is a great adjunct for patients with moderate OA.”
Early Identification and Interventions
Not everyone is a candidate for total knee replacement just because they have pain and disability. Many patients with knee OA can improve function, reduce pain, and increase range of motion with physical activity and physical therapy. The key is to identify patients early in the course of the disease and provide appropriate treatments that prevent OA progression and joint symptoms from getting worse. Although many patients wait until they have a substantial disability before seeking medical care, clinicians should encourage patients to talk to their physician or physiotherapist as soon as they begin to develop knee pain. Early identification and treatment are important aspects of reducing the burden of OA for the aging population.
Interventions in physiotherapy for patients with early or moderate OA often focus on two main targets: 1) reducing pain and symptoms associated with OA and 2) reducing the risk of structural OA progression. The first category is often accomplished with modalities and targeted exercises. For example, a patient with a painful and swollen joint may benefit from compressive wrappings and elevation to reduce the painful OA flare before performing physical activity. Suppose a patient has complaints of difficulty with stair climbing and is found to have muscle weakness. In that case, they may be given a progressive strengthening regimen that targets the quadriceps and gluteus muscles. While these interventions may improve the patient’s function and pain, they likely will not change the course of OA progression.
[sidebar float=”left” width=”250″]Product Resources
The following companies provide products for pain management:
Amrex Electrotherapy Equipment
www.amrexusa.com
Ari-Med Pharmaceuticals
www.ari-med.com
Battle Creek Equipment Company
www.battlecreekequipment.com
OPTP
www.optp.com
Parker Laboratories
www.parkerlabs.com
PHS Medical by Pivotal Health Solutions
www.phsmedicalsolutions.com
Sore No More
www.sorenomore.com
Southwest Technologies
www.elastogel.com[/sidebar]
Pain Management Toolkit
When temporary relief from pain symptoms may be called for, physical therapists have a variety of non-addicting, non-invasive approaches they may use. Transcutaneous electrical nerve stimulation, for example, transmits low-voltage electric current through the skin to activate endorphins that subsequently block the perception of pain. Electrical stimulation (E-Stim) devices are another tool that provide temporary pain relief, which send electrical pulses through the skin that block pain signals from reaching the brain. Both TENS and E-Stim can be used to temporarily relieve arthritis pain. Another option for short-term relief are topical analgesics formulated in gels, creams, and sprays. Topical analgesics provide an affordable treatment solution to penetrate the skin and modulate an individual’s perceived level of pain. Several sources offer topicals to the PT market, including Sore No More, Moab, Utah, which offers Sore No More Natural Pain Relieving Gels for warm therapy and cooling therapy. Other sources include Ari-Med Pharmaceuticals, Tempe, Ariz, and China Gel, Arlington Heights, Ill.
The second category of treatments, known as disease-modifying interventions, are focused on reducing further cartilage, muscle, and bone damage in and around the joint. Given the relationships between abnormal movement patterns and OA and obesity and OA, disease-modifying treatments usually target these areas. For example, a patient with apparent structural malalignment that places them in an excessive valgus, or knock-kneed, position may benefit from an unloader brace that restores a more normal alignment in the knee. Other interventions, such as shoe wedges, can also change the location of forces under the leg. These wedges can be customized to reduce knee forces in a specific manner that coincides with the patient’s X-rays or area of pain. Several extensive epidemiological and clinical studies have shown a clear benefit of reducing body weight on a patient’s knee joint. For example, in one large study, losing 5 kg of body weight was associated with a 50% reduction in the risk of developing knee OA. For patients who already have OA, clinical studies have shown that the more weight one can lose, the greater benefits in function and pain.
Movement Training Option
Gait retraining is another mechanism that physiotherapists can use to change the loads in and around the knee joint. Patients can be instructed and taught to move differently to reduce excessive loading at the knee. This may be accomplished by leaning the trunk, changing the toe-out angle, stabilizing the pelvis, or focusing on keeping a neutrally aligned knee when walking. While gait retraining results are mixed, more recent studies have shown that targeted interventions show the best likelihood of success. In other words, movement retraining should be individualized and patient-specific. General movement retraining programs may not capture the individual nuances that place a patient at risk for developing knee OA. If a patient is placed in a movement retraining program, their specific movement deficits should be addressed.
Traditionally, identification of movement deficits has been performed by having the clinician observe the patient walk down a hallway several times. While a clinician may be able to see substantial biomechanical asymmetries, visual assessment of movement is insufficient to capture the small abnormalities in the movement that occur in all three dimensions. Deficits such as varus thrust—one of the most important risk factors for OA—as well as tibial rotations and other subtle mechanical risk factors, are very difficult to identify from visual assessment. Tools that objectively quantify three-dimensional motion are needed to provide an accurate biomechanical diagnosis.
“Having tangible diagnostic information to form an accurate biomechanical solution for pain in a patient’s knee is vital, but even more valuable is a path to slow and manage Osteoarthritic knee dysfunction,” says Luis Zuniga, president of FYZICAL Therapy and Balance Centers, El Paso, Tex. “We know exercise is medicine. A therapist has never had greater tools to prescribe the dose.”
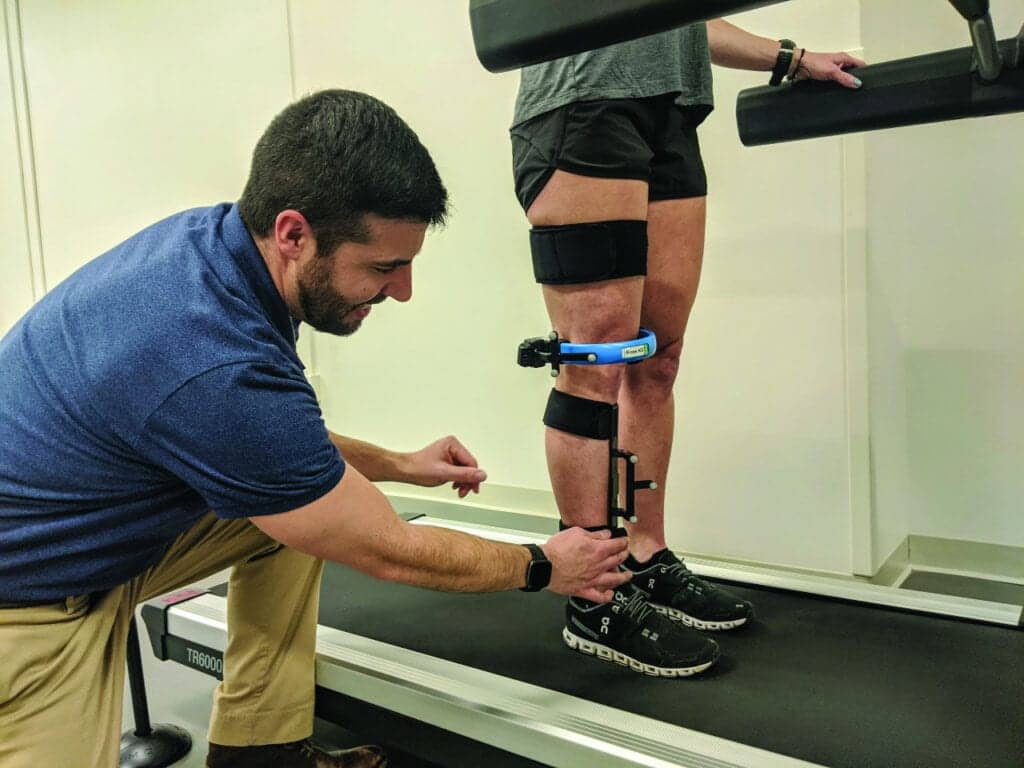
Motion Analysis and OA Management
Objective biomechanical measurements have previously only been available to researchers in motion analysis laboratories; however, commercially available tools are becoming available to the public. Thanks to the extensive work done by academic institutions, including the Centre hospitalier de l’Université de Montréal and École de technologie supérieure in Canada, devices such as the KneeKG enable a very accurate assessment of knee biomechanics and can identify risk factors, such as varus thrust. Clinicians are now using this device in clinical settings to identify movement abnormalities and prescribe patient-specific treatments for knee OA. A recent randomized clinical trial suggests that adding a knee kinesiography exam to the management of OA patients helped improve clinical outcomes. Clinicians could tailor the treatment plan based on individual deficits, which enhanced treatment adherence, improved functional outcomes and biomechanical measures, and increased patient and provider satisfaction with care.
Joint Replacement: Prehab & Rehab
Many patients with knee OA do eventually require total joint replacement. This surgery is extremely successful at reducing the pain and symptoms associated with end-stage knee OA. In preparation for surgery, many surgeons have patients undergo prehabilitation. This is a structured exercise program that aims to improve the strength and range of motion before surgery. One of the best predictors of postoperative outcomes is preoperative status. The stronger, more functional, or more flexible a patient is before surgery, the stronger, more functional, or more range of motion they will have after surgery. While there is no standard and universally adopted prehabilitation program, elements of a successful program include progressive lower extremity strengthening, range of motion exercises, and physical activity for conditioning and weight loss.
In addition to exercise, a prehabilitation program should also contain educational and planning components. Preoperative planning can include informing the patient of what type of assistive devices and adaptive equipment may be needed. A raised toilet seat, for example, is an excellent tool for patients who return home after surgery, especially for patients who have both knees replaced at the same time. Bending the knees is often the most painful and difficult task for patients after joint replacement. The raised toilet seat reduces the burden on the patient and caregiver and makes daily living activities much easier and safer. Other education aspects include setting appropriate expectations, informing them of postoperative exercises, and instructing a patient about how to arrange furniture in and around the house to make the patient more comfortable and less likely to fall.
Almost all patients after knee replacement participate in some form of rehabilitation. This may include a formalized outpatient physical therapy experience or a home exercise program supervised and reviewed by a physical therapist. The needs will vary depending on the patient’s age, goals, and functional status before and after surgery. Like prehabilitation, the focus of postoperative interventions includes improving strength, range of motion, and functional ability. There is also evidence to support the need for movement retraining after knee replacement. One recent study found that patients who undergo unilateral knee replacement and continue to walk with stiff-legged movement patterns are at greatest risk of needing the other knee replaced in the future.
Coping with the OA Continuum
There is clear evidence that exercise, weight loss, and physical activity is beneficial for patients early in the course of the disease, as well as for those who are scheduled for or who have undergone knee replacement. More importantly, it is crucial to detect and diagnose biomechanical risks factors such as the varus thrust with accurate tools to help prevent OA progression. Encouraging patients to seek medical care early in the course of the disease may help change their disease trajectory and delay or prevent knee replacement in the future. PTP
Joseph A. Zeni, Jr, PT, PhD, is an Associate Professor at Rutgers University. He received his PhD from the University of Delaware and his Masters from Quinnipiac University. Zeni has authored numerous publications in the areas of biomechanics and osteoarthritis. His work has been recognized with the Eugene Michels New Investigator Award from the APTA. For more information, contact [email protected].
This article originally appeared in the February/March Physical Therapy Products titled: Knee Osteoarthritis Pain and Treatment.
sidebar:
SEMG Biofeedback for Pain Management
By Geva Antopolsky, BPT
Pain is a complex experience. It has so many variables and dependencies, it would be simplistic and unrealistic to say there is one tool or method that is best for treating it. Pain management must take a multidisciplinary, multifaceted approach, combining many interventions and pain-relieving techniques.
One important facet is muscle conditioning. Pain is often triggered by biomechanical deficits, such as elevated muscle tone (think stress headaches, pelvic floor pain, TMJ dysfunction) or poor control of muscle activation in function, lack of coordination between muscle groups, and loss of contraction force and recruitment (patellofemoral pain, back pain, impingement syndromes, to name a few examples). Moreover, prolonged pain may result in further deteriorations in muscle function.
Utilizing the awesome power of biofeedback to help recondition, gain better control, strengthen, and learn to relax these muscles is easy, safe, efficient, and beneficial.
SEMG biofeedback is a simple, non-invasive modality that picks up electrical activity in skeletal muscles, augments, and reveals this otherwise imperceptible information. Information about neuromuscular electrical activity levels and timings gives the clinician insight about the system’s health and condition; the patient’s ability to contract, relax, and control muscle groups; and the underlying causes for symptoms, such as weakness, ataxia, hypertonicity, incontinence, and of course, pain. Quantifying activation levels, recording assessments and trainings, and comparing over time give clinicians an important means of keeping tabs on treatment progression.
Perhaps more importantly, once assessments are carried out, and dysfunctions and deficits are recognized, the feedback is used by the patient to identify, localize, and learn how to control function voluntarily. Good, timely, meaningful feedback is a basic principle in motor learning and rehabilitation of damaged and lost function. SEMG biofeedback is a superb means for doing this. Modern devices such as the MyOnyx by Thought Technology, Montreal, even have smart app operation and extravagant, entertaining features and feedback types, such as animations, games, music, and patterns, allowing the patient to understand and enjoy learning and training these functions, thus improving patient adherence and results.
A key factor in pain management is patient empowerment, shifting the focus to active involvement and helping the patient “get behind the wheel” and take charge of their rehabilitation.
This is exactly what SEMG biofeedback does. It is the epitome of “giving the keys” to the patient. By showing them, in real time, their activation and effort levels, you essentially give them all the information they need to train and improve on their own, by actively practicing and exercising. PTP



